2023年度中华医学科技论文TOP100
(编号364)
Mechanical ventilation (MV) is an essential life support method for patients with acute respiratory distress syndrome (ARDS), which is one of the most common critical illnesses with high mortality in the intensive care unit (ICU). A lung-protective ventilation strategy based on low tidal volume (LTV) has been recommended since a few years; however, as this did not result in a significant decrease of ARDS-related mortality, a more optimal ventilation mode was required. Airway pressure release ventilation (APRV) is an old method defined as a continuous positive airway pressure (CPAP) with a brief intermittent release phase based on the open lung concept; it also perfectly fits the ARDS treatment principle. Despite this, APRV has not been widely used in the past, rather only as a rescue measure for ARDS patients who are difficult to oxygenate. Over recent years, with an increased understanding of the pathophysiology of ARDS, APRV has been reproposed to improve patient prognosis. Nevertheless, this mode is still not routinely used in ARDS patients given its vague definition and complexity. Consequently, in this paper, we summarize the studies that used APRV in ARDS, including adults, children, and animals, to illustrate the settings of parameters, effectiveness in the population, safety (especially in children), incidence, and mechanism of ventilator-induced lung injury (VILI) and effects on extrapulmonary organs. Finally, we found that APRV is likely associated with improvement in ARDS outcomes, and does not increase injury to the lungs and other organs, thereby indicating that personalized APRV settings may be the new hope for ARDS treatment.
(编号391)
Background
The coronavirus disease 2019 (COVID-19) is an ongoing pandemic. Invasive mechanical ventilation (IMV) is essential for the management of COVID-19 with acute respiratory distress syndrome (ARDS). We aimed to assess the impact of compliance with a respiratory decision support system on the outcomes of patients with COVID-19-associated ARDS who required IMV.
Methods
In this retrospective, single-center, case series study, patients with COVID-19-associated ARDS who required IMV at Zhongnan Hospital of Wuhan University, China, from January 8th, 2020, to March 24th, 2020, with the final follow-up date of April 20th, 2020, were included. Demographic, clinical, laboratory, imaging, and management information were collected and analyzed. Compliance with the respiratory support decision system was documented, and its relationship with 28-day mortality was evaluated.
Results
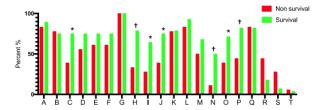
The study included 46 COVID-19-associated ARDS patients who required IMV. The median age of the 46 patients was 68.5 years, and 31 were men. The partial pressure of arterial oxygen (PaO2)/fraction of inspired oxygen (FiO2) ratio at intensive care unit (ICU) admission was 104 mmHg. The median total length of IMV was 12.0 (interquartile range [IQR]: 6.0–27.3) days, and the median respiratory support decision score was 11.0 (IQR: 7.8–16.0). To 28 days after ICU admission, 18 (39.1%) patients died. Survivors had a significantly higher respiratory support decision score than non-survivors (15.0 [10.3–17.0] vs. 8.5 (6.0–10.3), P = 0.001). Using receiver operating characteristic (ROC) curve to assess the discrimination of respiratory support decision score to 28-day mortality, the area under the curve (AUC) was 0.796 (95% confidence interval [CI]: 0.657–0.934, P = 0.001) and the cut-off was 11.5 (sensitivity = 0.679, specificity = 0.889). Patients with a higher score (>11.5) were more likely to survive at 28 days after ICU admission (log-rank test, P < 0.001).
Conclusions
For severe COVID-19-associated ARDS with IMV, following the respiratory support decision and assessing completion would improve the progress of ventilation. With a decision score of >11.5, the mortality at 28 days after ICU admission showed an obvious decrease.